As a part-time SEO Specialist with 3 years of experience in keyword ranking, on-page optimization, and data-driven SEO strategies, Aubrey specializes in on-page SEO—focusing on improving organic performance through well-structured content and precise optimization. By aligning content with search intent, Aubrey strengthens website foundations that lead to faster, more stable rankings.
Nasal obstruction refers to difficulty breathing through one or both nostrils. Common causes include deviated nasal septum, enlarged turbinates, nasal polyps, and allergic rhinitis. ENT doctors diagnose nasal obstruction using nasal endoscopy. Treatment options range from medical management (nasal steroid sprays, antihistamines) to surgical procedures such as septoplasty or turbinate reduction.
Key Takeaways
Definition: Difficulty breathing through one or both nostrils, constant or intermittent.
Common causes: Deviated nasal septum, enlarged turbinates, nasal polyps, allergies.
Diagnosis: Nasal endoscopy (small camera through the nostril) identifies the cause.
Treatment ladder: Medical management first (sprays, antihistamines). Surgery only if medical therapy fails.
When to see an ENT doctor: Persistent obstruction despite 4-8 weeks of medical treatment, or if obstruction affects sleep or quality of life.
Disclaimer:This information is for educational purposes only and does not constitute medical advice. Individual results vary. Please consult a qualified health practitioner for personal advice about your condition.
What Is Nasal Obstruction?
Nasal obstruction is the sensation of difficulty breathing through one or both nostrils. It may be:
Constant (always present) or intermittent (comes and goes)
Unilateral (one side only) or bilateral (both sides)
Positional (worse when lying down)
Nasal obstruction is not a disease itself but a symptom of an underlying condition affecting the nasal passages. The obstruction may result from structural problems (blockage) or inflammatory problems (swelling of the nasal lining).
Unlike a simple “stuffy nose” from a cold (which resolves in 7-10 days), chronic nasal obstruction persists for weeks or months and may require medical or surgical treatment.
Past medical history (allergies, asthma, previous nasal surgery or trauma)
Medication use (overuse of decongestant sprays)
2. Nasal Endoscopy
This is the most important diagnostic procedure. The doctor passes a thin, flexible tube with a small camera and light through the nostril. It takes 1-2 minutes and causes mild discomfort but is not painful.
What the doctor looks for:
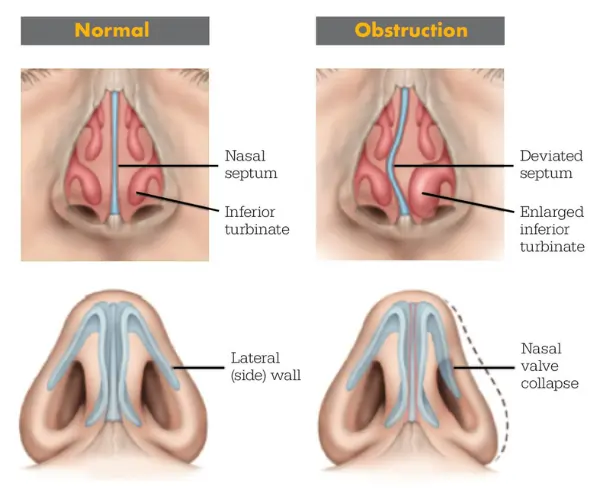
Deviated septum (the wall is bent to one side)
Turbinate enlargement (turbinates filling the nasal passage)
Nasal polyps (smooth, pale growths)
Nasal valve collapse (side wall sucks in during breathing)
Adenoid enlargement (in children, seen through the nose)
Tumours or foreign bodies (rare)
3. CT Scan (Selected Cases)
A CT scan may be ordered if:
The cause is not clear on nasal endoscopy
Chronic sinusitis is also suspected
Surgery is being planned
A tumour or complication is suspected
4. Allergy Testing
If allergic rhinitis is suspected, the doctor may recommend:
Skin prick testing (small amounts of allergens placed on the skin)
Treatment follows a stepwise approach – starting with medical management and progressing to surgery only if medical therapy fails.
Medical Management (First-Line Treatment)
Treatment
How It Works
Typical Duration
Intranasal corticosteroid sprays
Reduces inflammation and swelling (e.g., Flixonase, Nasonex, Rhinocort)
Daily, 4-8 weeks minimum
Saline nasal rinses
Clears mucus and allergens
Daily or twice daily
Antihistamines
For allergic causes (oral or nasal sprays)
As needed or daily
Decongestant sprays
Short-term relief only (e.g., Otrivin)
Maximum 3-5 days (risk of rebound congestion)
Oral decongestants
Systemic relief (e.g., pseudoephedrine)
Short-term use only
Allergy immunotherapy
Desensitization to allergens (drops or injections)
3-5 years
Warning: Decongestant nasal sprays (e.g., Otrivin, Sudafed spray) should not be used for more than 3-5 consecutive days. Longer use causes rhinitis medicamentosa (rebound congestion), making the obstruction worse.
Surgical Treatment (When Medical Therapy Fails)
Surgery is recommended when:
Medical management has failed after 4-8 weeks of optimal treatment
A structural cause (deviated septum, enlarged turbinates) is identified on nasal endoscopy
The obstruction significantly affects sleep, exercise, or quality of life
Surgical Procedures for Nasal Obstruction
Procedure
What It Does
Recovery Time
Septoplasty
Straightens the deviated nasal septum
1-2 weeks off work; full healing 4-6 weeks
Turbinate reduction
Reduces size of enlarged turbinates (radiofrequency, coblation, or microdebrider)
3-7 days off work; some congestion for 2-4 weeks
Nasal valve repair
Strengthens the side wall of the nose
1-2 weeks off work
Polypectomy
Removes nasal polyps (if present)
3-7 days off work
Important notes about surgery:
Procedures are performed through the nostrils (no external incisions)
Usually performed under general anaesthesia
Most patients return to work within 1 week
Full improvement in breathing takes 4-6 weeks (after swelling resolves)
Seek immediate medical attention (emergency department or call 000) if you experience:
Sudden onset of unilateral nasal obstruction with facial swelling or eye symptoms
Nasal obstruction after facial trauma (possible nasal fracture)
Bloody nasal discharge with persistent obstruction (especially unilateral)
Associated double vision, vision changes, or severe headache
These symptoms may indicate a nasal tumour, nasal fracture, or infection spreading to surrounding tissues.
Frequently Asked Questions (FAQs)
General FAQs
What is the most common cause of nasal obstruction? The most common causes are deviated nasal septum (structural) and allergic rhinitis (inflammatory). Many patients have both.
Can nasal obstruction be caused by allergies? Yes. Allergic rhinitis causes swelling of the nasal lining, leading to obstruction. Treating allergies often improves breathing.
Is nasal obstruction dangerous? Rarely. Chronic nasal obstruction affects quality of life (sleep, exercise, concentration) but is not usually dangerous. However, unilateral persistent obstruction in adults should always be evaluated to exclude a tumour.
Can nasal obstruction go away on its own? It depends on the cause. Obstruction from a cold resolves in 7-10 days. Obstruction from a deviated septum or enlarged turbinates does not resolve without treatment.
How do ENT doctors diagnose the cause of nasal obstruction? Using nasal endoscopy – a small camera passed through the nostril to directly visualise the septum, turbinates, and nasal passages.
Treatment FAQs
Can nasal obstruction be treated without surgery? Yes. Medical management (nasal steroid sprays, saline rinses, antihistamines) is the first-line treatment. Surgery is only recommended if medical therapy fails.
How long does it take for nasal steroid sprays to work? Nasal steroid sprays take 4-8 weeks of daily use to reach maximum effectiveness. Many patients stop too early.
Is septoplasty painful? The surgery is performed under general anaesthesia (no pain during). Mild to moderate discomfort during the first week of recovery is normal and managed with pain relief medication.
What is the success rate of septoplasty? Studies show 80-90% of patients experience significant improvement in nasal breathing after septoplasty.
Can a deviated septum get worse over time? Not usually. The deviation is stable. However, aging changes or trauma may worsen symptoms.
Recovery FAQs
How long is recovery after nasal surgery? Most patients return to non-physical work within 1 week. Full healing and maximum breathing improvement takes 4-6 weeks.
Will I have nasal packing after surgery? Some surgeons use soft silicone splints (removed at 1 week). Traditional nasal packing (gauze) is less common now.
Can I fly after nasal surgery? Avoid flying for 2-4 weeks after surgery (air pressure changes can cause bleeding or pain).
Will septoplasty change the shape of my nose? No. Septoplasty straightens the inside of the nose. It does not change the external appearance unless combined with rhinoplasty (cosmetic nose surgery).
Can children have septoplasty? Septoplasty is usually delayed until facial growth is complete (around age 16-18 for girls, 18-20 for boys) unless the obstruction is severe.
Lifestyle FAQs
Does nasal obstruction cause snoring? Yes. Nasal obstruction is a common cause of snoring and may contribute to sleep apnoea.
Can exercise help nasal obstruction? Exercise temporarily constricts blood vessels in the nose, which may improve breathing during and shortly after activity.
Does nasal obstruction affect sense of smell? Yes. Chronic nasal obstruction reduces airflow to the olfactory nerves, leading to reduced sense of smell (hyposmia).
Is nasal obstruction linked to sleep apnoea? Yes. Nasal obstruction increases the risk of snoring and obstructive sleep apnoea. Treating the obstruction may improve sleep apnoea symptoms.
Can pregnancy cause nasal obstruction? Yes. Pregnancy rhinitis (hormonal swelling of the nasal lining) affects up to 30% of pregnant women. It resolves after delivery.
Summary
Nasal obstruction is difficulty breathing through one or both nostrils. Common causes include deviated nasal septum, enlarged turbinates, nasal polyps, and allergic rhinitis. ENT doctors diagnose the cause using nasal endoscopy.
Treatment begins with medical management (nasal steroid sprays, saline rinses, antihistamines) and may progress to surgical procedures such as septoplasty or turbinate reduction for patients who do not improve with medical therapy alone.
For specific medical advice about your condition, please consult a qualified ENT doctor in Sydney such as Dr. Brett Leavers or another registered ENT specialist.